Executive summary
- BA.1 infections do not provide complete protection against BA.2 infection: 146 out of 788 reinfections from the BA.2 wave occurred during the BA.1 wave.
- All things being equal, however, a patient last infected with a non-Omicron variant is still more likely to be reinfected today than a patient last infected with an Omicron variant.
- As vaccine and infection induced immunity wanes, mitigation measures ease, and SARS-CoV-2 evolution continues, we expect reinfections to become the norm.
Background
With the second Omicron wave well underway, a pressing question is whether prior infection during the Omicron BA.1 wave is protective against the current wave driven by Omicron BA.2. Although hospitalization and deaths are not increasing at alarming rates, a surge in cases may cause unanticipated and disruptive labor shortages. Moreover, each new covid infection carries the risk of long covid, which can lead to debilitating symptoms.
Data source
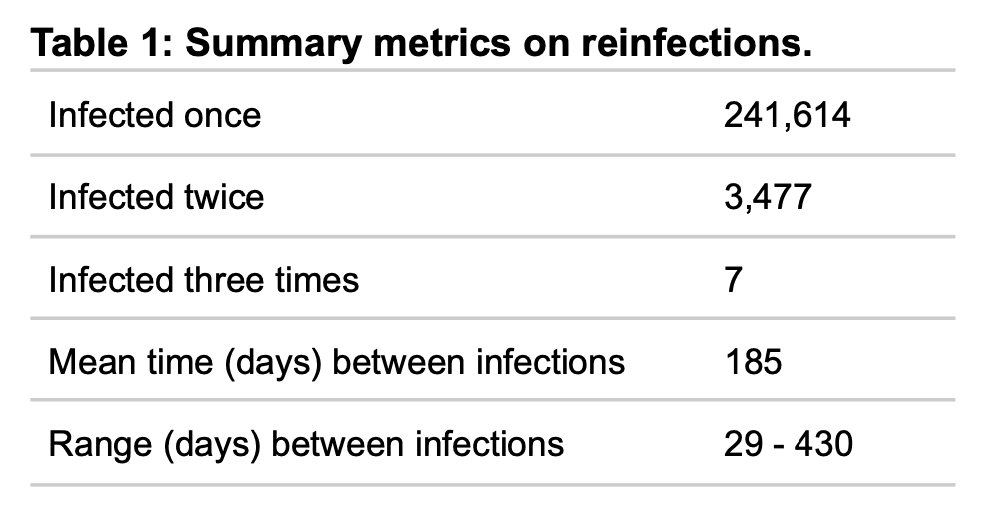
This analysis uses 304,771 SARS-CoV-2 positive test results from 245,098 unique individuals in the United States who have tested with Helix and received at least one positive result. To increase our sensitivity to reinfections, we define positive tests separated by more than 28 days as distinct infections (see Data Processing section). This resulted in 248,589 positive results, each considered to represent a unique infection. For the period from March 12, 2021 to May 21, 2022 there were 241,614 once-infected, 3,477 twice-infected, and 7 thrice-infected patients (Table 1). Not all positive cases are sequenced, therefore throughout this analysis, the timing of infection is used as a proxy for the infecting variant rather than the viral sequence.
Timing of previous infections
For each twice-infected individual, we examined the timing of their previous infection. To specifically address the question of Omicron reinfection, we limited the analysis to reinfections during the BA.1 wave (Jan & Feb 2022) and the current BA.2 wave (Apr & May 2022).
Figure 1 shows that for BA.1 reinfections, the timing of the corresponding first infection largely coincides with the Alpha and Delta surges (light blue solid line). For BA.2 reinfections, there are more first infections that occur during the BA.1 surge, though first infections during Alpha and Delta surges still predominate (dark blue dashed line).
Reinfections are correlated with surges in cases as well viral evolution and waning immunity. Thus, on the one hand, we expect to see BA.1/BA.2 reinfections because of the sheer numbers of BA.1 cases and because BA.1 and BA.2 are antigenically distinct. Relative to overall cases (Figure 1 pink line), BA.1/BA.2 reinfections are actually lower compared to Alpha/BA.2 or Delta/BA.2 reinfection. All else being equal, someone who was last infected with Alpha or Delta is more likely to be reinfected today than someone who was last infected with BA.1.
On the other hand, 146 out of 788 reinfections (18%) in the BA.2 wave occurred after January 2022. This is a much higher level of reinfection than would be expected a year ago, given the initial results on vaccine efficacy.
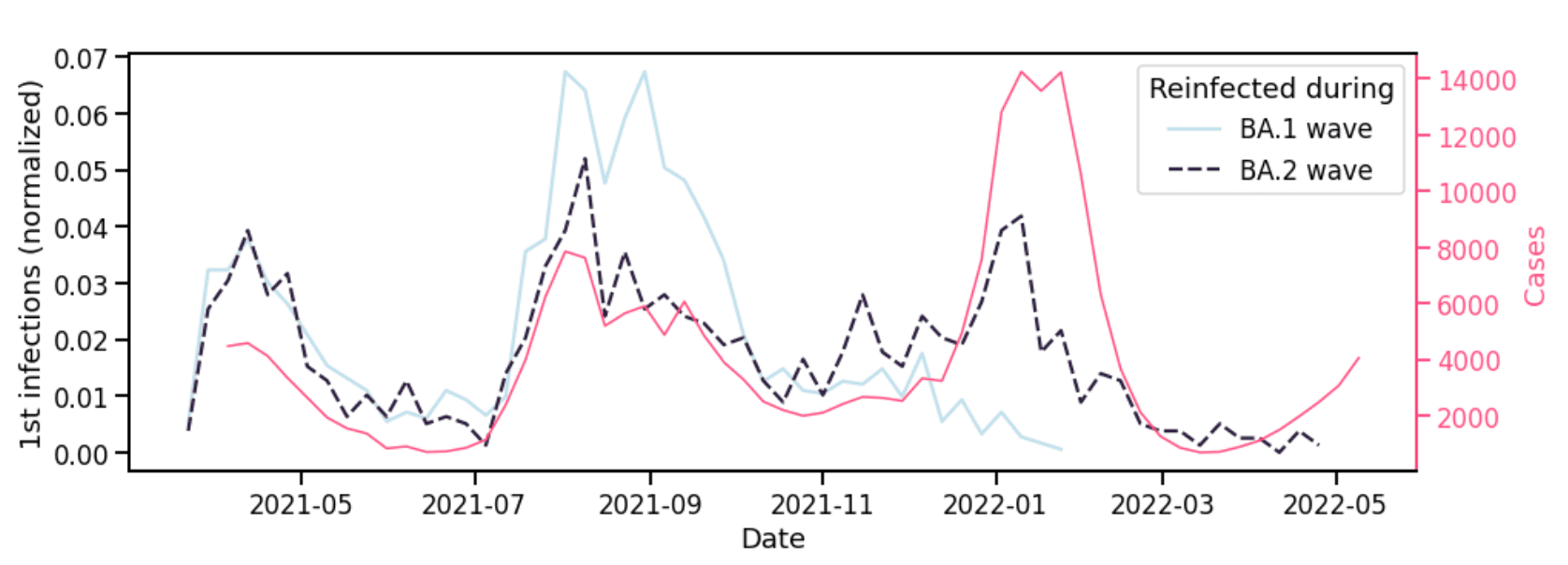
Figure 1. Timing of first infections corresponding to reinfections in the BA.1 and BA.2 waves. Left y-axis denotes, for each wave, the number of first infections per week normalized by the total reinfections during that wave. Right y-axis is the number of cases from Helix’s covid diagnostic testing operation.
Individuals infected three times with Omicron
Cases of individuals putatively infected three times since January 2022 demonstrate how BA.1 protection against BA.2 is far from absolute (Figure 2).
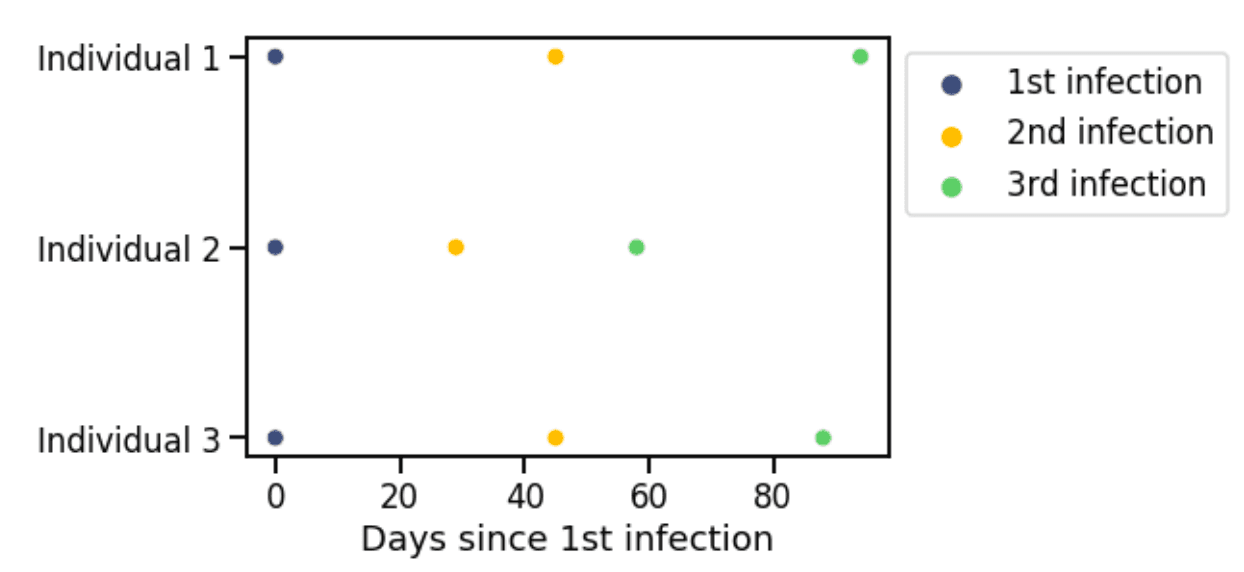
Figure 2. Patients infected three times since January 2022.
These thrice infected patients are likely edge cases for now. However, as mitigation measures such as masking ease, and as travel and indoor socializing increase, it will be important to understand whether we should expect frequent reinfection – i.e., within months – as an inevitable consequence of a resumption of pre-pandemic activities, or if such cases will remain rare. Prioritizing contact tracing efforts towards reinfected individuals could help identify the cause for high-frequency reinfections.
Caveats
This dataset does not include diagnostic test results reported by other providers, or that were obtained through at-home testing. These numbers are therefore an undercount of total infections, both of reinfections and of first infections. As such, we do not attempt to draw quantitative conclusions about the rate of reinfection. For example, we cannot simply calculate the reinfection rate as the fraction of total infections that are second infections: both tallies are undercounts in ways we are not able to model, at this time.
It should also be noted that the 4-week threshold for a ‘new’ infection is intended to increase our ability to detect rapid reinfection, even if it means mischaracterizing long-lived infections. Anecdotal accounts of reinfections a month after a previous infection motivated us to use the shorter period of 4 weeks, even though 90 days is the typical window within which the CDC does not require isolation after exposure, i.e. 90 days is the time frame within which reinfection is currently not expected.